WARNING: QT PROLONGATION and SUDDEN DEATHS See Full Prescribing Information for complete Boxed Warning. - Nilotinib prolongs the QT interval. Prior to DANZITEN administration and periodically, monitor for hypokalemia or hypomagnesemia and correct deficiencies. (5.3) Obtain ECGs to monitor the QTc at baseline, seven days after initiation, and periodically thereafter, and following any dose adjustments. (5.3, 5.4, 5.8, 5.12)
- Sudden deaths have been reported in patients receiving nilotinib. (5.4) Do not administer DANZITEN to patients with hypokalemia, hypomagnesemia, or long QT syndrome. (4, 5.3)
- Avoid use of concomitant drugs known to prolong the QT interval and strong CYP3A4 inhibitors. (7.1, 7.2)
|
ADDITIONAL IMPORTANT SAFETY INFORMATION
Contraindications
DANZITEN is contraindicated in patients with hypokalemia, hypomagnesemia, or long QT syndrome.
Warnings and Precautions
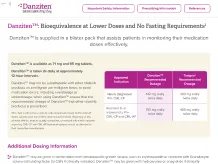
Substitution With Other Nilotinib Products and Risk of Medication Errors: DANZITEN tablets may not be substitutable with other nilotinib products, including other nilotinib tablets, on a milligram per milligram basis. Confirm that the intended nilotinib product is being prescribed and dispensed.
Myelosuppression: Monitor complete blood count (CBC) during therapy and manage by treatment interruption or dose reduction.
Cardiac and Arterial Vascular Occlusive Events: Evaluate cardiovascular status, monitor and manage cardiovascular risk factors during DANZITEN therapy.
Pancreatitis and Elevated Serum Lipase: Monitor serum lipase; if elevations are accompanied by abdominal symptoms, interrupt doses and consider appropriate diagnostics to exclude pancreatitis.
Hepatotoxicity: Monitor hepatic function tests monthly or as clinically indicated.
Electrolyte Abnormalities: DANZITEN can cause hypophosphatemia, hypokalemia, hyperkalemia, hypocalcemia, and hyponatremia. Correct electrolyte abnormalities prior to initiating DANZITEN and monitor periodically during therapy.
Tumor Lysis Syndrome: Maintain adequate hydration and correct uric acid levels prior to initiating therapy with DANZITEN.
Hemorrhage: Hemorrhage from any site may occur. Advise patients to report signs and symptoms of bleeding and medically manage as needed.
Fluid Retention: Monitor patients for unexpected rapid weight gain, swelling, and shortness of breath. Manage medically.
Effects on Growth and Development in Pediatric Patients: Growth retardation has been reported in pediatric patients treated with nilotinib. Monitor growth and development in pediatric patients.
Embryo-Fetal Toxicity: Can cause fetal harm. Advise females of reproductive potential of potential risk to a fetus and to use effective contraception.
Treatment Discontinuation: Patients must have typical BCR-ABL transcripts. An FDA-authorized test with a detection limit below MR4.5 must be used to determine eligibility for discontinuation. Patients must be frequently monitored by the FDA authorized test to detect possible loss of remission.
Adverse Reactions
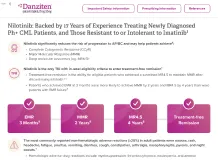
The most commonly reported non-hematologic adverse reactions (≥20%) in adult patients are nausea, rash, headache, fatigue, pruritus, vomiting, diarrhea, cough, constipation, arthralgia, nasopharyngitis, pyrexia, and night sweats. Hematologic adverse drug reactions include myelosuppression: thrombocytopenia, neutropenia, and anemia.
These are not all the possible side effects of DANZITEN. Please see Full Prescribing Information for a full list.
Drug Interactions
Strong CYP3A Inhibitors: Avoid concomitant use, including grapefruit juice with DANZITEN or reduce DANZITEN dose if concomitant use cannot be avoided.
Strong CYP3A Inducers: Avoid concomitant use with DANZITEN.
Proton Pump Inhibitors: Use short-acting antacids or H2 blockers as an alternative to proton pump inhibitors.
See Full Prescribing Information for Specific Drugs and Interactions.
Use in Specific Populations
Lactation: Advise women not to breastfeed.
Pediatric Use: The safety and effectiveness of nilotinib in pediatric patients below the age of 1 year with newly diagnosed, or who are resistant to or intolerant to Ph+ CML in chronic phase and accelerated phase have not been established.
The Important Safety Information does not include all the information needed to use DANZITEN safely and effectively. Please see Full Prescribing Information for DANZITEN.
To Report SUSPECTED ADVERSE REACTIONS, contact Azurity Pharmaceuticals, Inc. at 1-800-461-7449, or FDA at 1-800-FDA-1088 or www.fda.gov/MedWatch.